
Sexually Transmitted Infections (STIs) and Safe Sex
Have Fulfilling Love and Intimacy without Getting Infected—
by Understanding What's Going On and What to Do About It
(and using a fair bit of good judgment and self-restraint)
I compiled this fact sheet because people I care about, in part through a lack of accurate information about the current specifics of sexually transmitted diseases and how to avoid them, are getting hurt.
One had only two sex partners in her life, was fairly selective and careful, but still contracted a sexually transmitted infection in her early twenties (not fair!). Another I carried to the car and drove to the hospital in the middle of the night, with blood pouring out of her. Another, also in her early twenties, also with pretty good judgment, caring, educated parents, sex ed in school, at home etc. etc. just had an irregular pap smear and is facing the prospect of cervical cancer, awkward conversations with prospective partners, etc.
The challenges my parents faced in dodging this particular obstacle to finding fulfilling love and intimacy in the in the 1950s, and the ones I faced in the 1980s are vastly different to those my children and young friends are facing in the 2010s.
The more people get this hazard in focus and act effectively to avoid it, the better and easier it will be for everyone.
I am appalled at:
1) how virtually all sources of information fail to convey the staggering change in risk in the past 40 years
2) how little practice (or even discussion) there is of sexual behavior that is adapted to avoiding health issues while still fulfilling intimacy needs under the new conditions
Almost everyone who reads this is shocked when they realize how out of touch their understanding and behavior is with the static's on what’s happening:
In the United States, more than 65 million people are currently (2009) living
with an incurable sexually transmitted disease (STI). An additional 15 million
people become infected with one or more STIs each year, roughly half of whom
contract lifelong infections. The average sexually transmitted infection rate
is at 50% of young Americans, and climbing rapidly. Yet, STIs are one of the
least recognized health problems in the country today.
The U.S. has the highest STI rates of any country in the industrialized world. Despite this, there is no national campaign to promote the prevention, treatment and cure of these infections.
Why isn’t this on the news every night?
With infection rates this high, unprotected intercourse is like playing Russian roulette with bullets in three of the six chambers. How many times is it advisable to do this? Once? Twice? Not much more than that.
This is a Radical change in forty years. To have a 50% chance of contracting a sexually transmitted infection that will be with you until the day you die, you would have to exchange body fluids with something like:
= 1000 people in 1967
= 40 people in 1987
= 4 people in 2007
[my estimates; this depends on many factors and could be off by a factor of two]
Our culture is barely becoming aware of this drastic shift, let alone adapting to it with behavior change. The information in the air—from movies, books, peers—is almost entirely formed under 1970’s conditions, and works counter to currently sensible behaviors. In the AIDS epidemic, the “golden boys”—the most beautiful, desirable, successful men, who could sleep with anyone they wanted, were the first to go. Today the golden people are not dying, in fact they are mostly asymptomatic, but it safe to say that with average infection rates of 50% for young Americans, the majority of the hottest young folk are carriers of a range of incurable STIs. Our culture has scarcely begun to take this reality into account, let alone develop a culture of appropriate behavior.
Note: this information
is based on a combination of internet research in early 2009, direct personal
experience, and conversations with others, as well as memory of studies I’ve
read, etc, some of which are three decades old. I think that the overall gist of this is accurate and more
useful than most of what’s out there. However, this or that individual data
point may not be accurate, as it has not been peer reviewed or exhaustively
cross-checked. It doesn’t matter
for the core points here that, for instance, that the summer of love was in
1967, not 1969, or that condoms reduce risk 80% or 90%. “Better
roughly right than precisely wrong”…but, if your application requires accuracy
in this or that detail, double check.
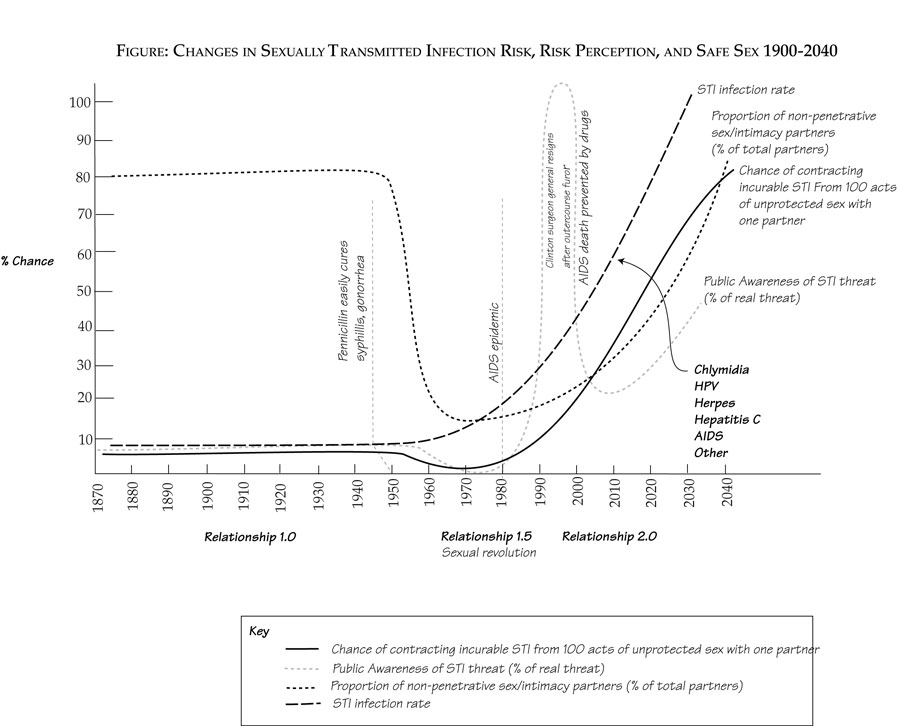
Right now is the time of maximum peril: danger is high, and awareness is low. In the future, awareness will have caught up, and behavior will have adapted.
It’s a pretty tough dilemma; desire for intimacy and satisfaction on one side, versus self preservation (guarding against permanent physical damage or death) on the other.
Here’s the options, in descending order of safety:
1. Total celibacy
2. Only have sex sith virgins
3. Enjoy non-sexual physical intimacy (massage, dance, hugging, etc.)
4. Save unprotected sex for a very, very few long-term relationships, screened through a rigorous requirement that you wait to have unprotected sex with someone until you’ve known them a long time (a year? Five years?), and with extensive, open discussion of their sexual history and their partner’s sexual history, and testing
5. Have outercourse (sex without exchange of body fluids)
6. Use condoms rigorously (still has 15%± chance of infection)
7. Relax...and probably get infected for life with one thing after another
My assessment is that a combination of options 3-6 is optimal; the closest thing to a solution to a problem that doesnt' have an entirely satisfactory solution.
In our culture, there is a bright, narrow line between non-sexual relations and sexual relations, which are thought to equal sexual intercourse. It is true that if you just get rushed across in a hurry, it seems like a narrow line. But, if you take the time to linger, you’ll find that it is a lot broader and fuzzier than that. Warmer, too. In fact, the longer you hang out there, the more you’ll realize it is such a vast and rich a garden of pleasure that one could never hope to explore all of it in a single lifetime.
The trick is that this requires quite a bit of self-restraint (and quite possibly requiring that someone you care about exercise restraint as well). This isn’t necessarily easy to do when you’re sparking strongly with someone. But, considering the options, this restraint is something our culture is would do well to get a lot better at in the future.
What to Do
"Though I'm completely open to you and desirous of you, it is my policy to have completely safe sex until/ unless [fill in blank how you wish; we find our proven, long-term stable footing together, for six months, whatever ...]"
Also...if you have an STI or STIs, you can seek out others who have the same---if everyone did this, this would stop the spread of STIs in their tracks.
The rest of this article is gleanings of interest from the internet on STIs and safe sex, with commentary, and a bit of original writing.
Facts & Figures Highlights:
More than half of all sexually active teens have never discussed STIs with their partner or
health-care provider.
Most Americans underestimate their risk of getting an STI. According
to recent survey data, only 14
percent of men and 8 percent of
women think they are at risk of
becoming infected. Because the risk is underestimated — and because many
STIs are “silent” in their early
stages — many people do not get tested and then inadvertently pass the infection to others. Lack of STI awareness is
perpetuated by stigma, secrecy and
shame, even between health-care
providers and patients. Over half of all adults and over one-third of all teens
in 1995 said that their
health-care providers spent no time discussing STIs with them.
This epidemic is a recent phenomenon. Some young people have parents
who may have had multiple sexual partners with relative impunity. They may
conclude that they too are safe from disease. However, most of these diseases
were not prevalent 20 to 30 years ago. Prior to 1960, there were only two
significant sexually transmitted diseases: syphilis and gonorrhea. Both were
easily treatable with a short course of antibiotics.
A study from Florida looked at couples
where one individual was HIV positive and the other was negative. They used
condoms as protection during intercourse. Obviously these couples would be
highly motivated to use the condoms properly, yet after 18
months, 17% of the previously uninfected partners were now HIV positive. That
is a one-in-six chance, the same as in Russian roulette. Not good odds!
Safe sex means making sure you don't get anyone else's blood, semen, vaginal fluids, or breast milk in your body.
Talk smart sex first. Have smart sex later. STIs and unintended
pregnancies affect both partners, not just one person. If you feel
uncomfortable discussing sex and birth control with your partner, then you shouldn't
be having sex.
Respect everyone's right to make his/her own personal decision -
including yourself. There is no imaginary "deadline," no ideal age,
no perfect point in a relationship where sex has to happen.
The difficult part of outercourse is the temptation of intercourse.
This is especially acute if/ when both partners want it at the same time, or if
one partner becomes so obsessed with intercourse desire it spoils the enjoyment
of anything else. If orgasm can be achieved without succumbing to intercourse,
you’re probably out of the woods…for a while.
History
The sexual revolution
The sexual revolution was a one-time,
probably never to be repeated event. It was brought about by the unique
confluence of general social revolution and two new technologies: penicillin,
and the pill.
Fear of pregnancy, when that used to
mean that the woman would be stuck with the child, and probably the father as
well, was the main motivator for abstinence and non-penetrative sex. Even with
condoms, one out of ten women will get pregnant in a single year of sex. How
many years of sexual prolificacy does it make sense to have with these odds?
The birth control pill eliminated the
possibility of pregnancy, transparently, without the need for any awkward
conversations, fumbling with birth control devices, or behavior modification in
the moment of heat. (Legalized abortion also put a safety net under those who
couldn’t be bothered to take the pill).
Prior to and during the free sex era,
the only STIs of significance were syphilis and gonorrhea. With the advent of
widespread, affordable penicillin just after WWII, these went from being
horrible, lifelong and occasionally lethal diseases, to the inconvenience of a
doctor’s visit, a short course of penicillin, then back to the party...
Right as the rest of establishment
culture was being questioned, recreational drug use was becoming acceptable,
and women liberated, the consequences of wanton sex went from being serious and
life changing, to minor inconvenience.
For a few decades it seemed like there was
no compelling reason to not have sex with anyone one had the slightest desire to have
sex with.
Human nature being what it is, many,
many people did just that. The average number of unprotected sex partners
skyrocketed. Many people exchanged fluids with hundreds or even thousands of
partners. And virtually everyone got away with it, until…
The emotional consequences of multiple,
random sexual attachments became so undeniably severe that many people began to
question the viability of free love, without attachments.
And, in the 1980s the AIDS epidemic
flashed like wildfire through the gay population, and scared the beejeebers out
of everyone. Public wasting away and death, starting with the most attractive,
sexually active people, was such a spectacular consequence that it really got
people’s attention.
Behind the AIDS epidemic was the start
of a generalized epidemic of STIs that had never been very prevalent before.
People’s “Fluid exchange networks” became exponentially more extensive and
rapid. If someone had unprotected sex with one new person, they were also
effectively exchanging fluids with perhaps fifty or a hundred other people who
had exchanged fluids with that person. By this means, infections that had been in dozens of people were spread
to millions within ten years. Infections that were less likely than being
struck by lightning in 1967 now affect tens of millions of Americans, and in
some populations as likely to contract from a single act of unprotected sex as
flipping a coin and having it come up “tails.”
Americans excel at selling stuff with
sex, sexualizing everything in the process, down to inhumanly proportioned
kid’s dolls and thong underwear for grade schoolers. But, Americans are quite
prudish and ineffectual when it comes to really dealing with sex and its
consequences. This, and the success of the religious right in suppressing sex
education and contraception, has seriously hobbled efforts to respond
effectively to what by any measure constitutes a national emergency.
At this point, STIs are spreading and
mutating faster than treatments are being developed, and it will be many
generations, if ever, before this genie is back in the bottle.
The lovely resource of a population with low STI rates has been squandered.
What to do?
Making a decision
Is it worth the risk to have sex with this person?
The short answer, the one which you should have ready in the heat of the moment, is “no,”
It is not worth it to have unsafe sex, however hot, for a short-term liaison.
If you are using birth control (you should be) and willing to have an abortion as a back up, the physical risk is dominated by the chance of getting an incurable STI.(Protection from emotional risk is a whole other kettle of fish, for a different article a different day. It is worth noting however, that the emotional sting of things not working out is lessened without adding the injury of permanent infection to the insult of whatever led to the breakup. Also, emotional attachments to people take longer to become painfully deep without intercourse).
If you have unprotected, vaginal sex with 4 average guys, you've probably exposed yourself to two or three different STIs, and may have contracted one of them.
If you sleep with just one hot guy who's been taking advantage of their hotness to sleep with many women, you're risk is probably higher than with the 4 average guys, as there are dozens or hundreds of partners in their sexual network.
At current rates of infection, it probably makes sense to have unprotected sex with only one or two partners, and give the hot, promiscuous guys a pass, unless you want to marry them, infections and all.
If you have intense but non-sexual intimacy with 100 guys and gals, "outercourse" with 20 more, and protected sex with 5 carefully screened long-term partners, and manage to find a clean life partner for unprotected sex/ fathering your children who has been equally careful, your chances of infection total something like 50%, most of it from the condom-protected penetrative sex. If you skipped that part, your chance of infection is close to zero. This is about as good as it gets, short of time-machining your way back to 1967, after penicillin, but before the epidemic.
Questions to ask yourself and your prospective partner
If it feels
too awkward to have the whole sex talk in the beginning, delicate stages of the
relationship, Take this stand first
We are going
to enjoy totally, completely safe sex together until we know each other better
and longer. See “what is safe sex,” below
What do you
know about safe sex? (these two questions establish
how much you’re going to have to educate your partner on the basics before
moving on to these questions:
What do you
know about STIs?
Who is in your
fluid exchange network?—How many people have you
had unprotected sex with, and who have they had unprotected sex with? How high
risk are they? Virgins? Promiscuous Drug users?
Have you had
any symptomatic STIs?—If someone has had
urinary tract infections and other less serious infections that indicates a
high risk for other, asymptomatic but more serious infections. Because 75% of
common STIs are asymptomatic, the absence of symptoms does not mean they are
clean, however…
What have
you been tested for? When?
Can you name
which common STIs don’t show up on tests, their prevalence, and how to avoid
them, if possible?
What have
you done to protect yourself and your partners in the past?
Agree on
limits to exchange of fluids, things you’ll do and not do—see safe sex, below
Agree on
limits to exchanging fluids with other partners while you're together—see safe sex, below
If they show
signs of not respecting them in the heat of the moment, back off on the
intimacy.
STI Decision Wizard
This is an idea for a free, web-based tool, hosted by someone like Planned Parenthood, to shed light on the half of this bottom line: what's the risk of my having sex with this person?
The emotional risk is...well, not much you can do about that. The other half of the bottom line—what's the reward? Is something that you'll have to figure out more intuitively, considering how much the experience is likely to enrich your life experience, and for how long?
*The likelihood of contracting a lifelong infection from a single act of sex, or a year of sex with one partner, is the static that is most meaningful, and hardest to come up with, because it involves the synthesis of so much information.
1) The accuracy of the bottom line is dominated by the inaccuracy of the least accurate factor calculated into it. For example, the average infection rates for the more popular infections might be off by 30% due to underreporting and non-symptomatic, un-testable infections. But the transmission rates might be off 50%, because these have hardly been tested.
2) Your particular situation is not average. If you are a teenage woman, your infection chances are about 50% greater due to the physiology of your vagina. If your prospective partner is an uninhibited person who has been having sex with other uninhibited people, it is probably more a question of how many infections they have than if they have any.
This risk could be based on 100 sessions of unprotected vaginal sex. This is roughly a year for the average American couple. For a single act of sex, divide the risk by about ten (the risk increase is not linear; if you're going to get something from someone, it is more likely to happen in the first few sessions, and the additional between having sex with them 100 or 1000 times is a few percent more, not 10 times more. Consider that there's absolutely no point in having unprotected sex with someone you can't see being with for at least a year.
For condom use divide risk by 10.
Sexually Transmitted Infections—Research Notes
Fact Sheet: Sexually Transmitted Diseases in the United States
http://www.thebody.com/content/prev/art2447.htmlhttp://oasisdesign.net/health/sti/
October/November 2001
More than 25 diseases are primarily
spread through sexual activity. The trends for each disease vary considerably,
but together these infections comprise a significant public health problem.1
In
the United States, more than 65 million people are currently living with an
incurable sexually transmitted disease (STI). An additional 15 million people
become infected with one or more STIs each year, roughly half of whom contract
lifelong infections. Yet, STIs are one of the least recognized health problems
in the country today.2
While extremely common, STIs are difficult to track. Many people with
these infections do not have symptoms and remain undiagnosed. Even diseases
that are diagnosed are frequently not reported and counted. These "hidden" epidemics are magnified with each new
infection that goes unrecognized and untreated.3
Incidence and
Prevalence
* Chlamydia is the most commonly
reported infectious disease in the United States. Reported Chlamydia
rates in women greatly exceed those in men, largely because screening programs
have been primarily directed at women. True rates are probably far more similar
for women and men.9
* 75 percent of women and 50
percent of men with Chlamydia have no symptoms. The majority of cases
therefore go undiagnosed and unreported.14
* The reported gonorrhea rate in the United
States remains the highest of any industrialized country: roughly 50 times that
of Sweden and eight times that of Canada.18
* Ten to 20 percent of women with gonorrhea and
Chlamydia develop one of the most serious complications, pelvic inflammatory
disease (PID).19
* An estimated 70,000 people become infected
with syphilis each year in the United States.20
* An estimated 1 million people
become infected with herpes each year in the United States, and an estimated 45
million Americans are currently infected.24
* An estimated 5.5 million people
become infected with HPV each year in the United States, and an estimated 20
million Americans are currently infected.25
* There are 30 distinct types of HPV that can
infect the genial area. Of these, some types cause genital warts and others
cause subclinical infections.26
* An estimated 120,000 people become infected
with hepatitis B each year in the United States, and an estimated 417,000
Americans are currently infected.27
* Hepatitis B vaccinations have been recommended
for people with risk factors since the vaccine became available in 1981.28
* An estimated 5 million people become infected
with trichomoniasis each year in the United States.29
* No recent surveys of the estimated number of
people currently infected with gonorrhea, syphilis, trichomoniasis, or
bacterial vaginosis have been conducted.30
* Approximately 25 percent of all
new STI infections are in teenagers.31
* Young women are biologically more susceptible
to Chlamydia, gonorrhea, and HIV.32
* An estimated 75 percent of the reproductive-age population
have been infected with sexually transmitted HPV.33
* Infection with certain types of HPV place
women at increased risk for cervical cancer.34
* Research indicates that approximately one
percent of sexually active adults in the United States have genital warts.35
* More than one in five Americans -- 45 million
people -- are infected with genital herpes.36
* Herpes is more common in women, infecting
approximately one out of four, versus one out of five men.37
* Women who are infected with an STI while
pregnant can have early onset of labor, premature rupture of the membranes, or
uterine infections before and after delivery.38
* Multiple studies and surveillance projects
have demonstrated a high prevalence of STIs in persons entering jails and
juvenile detention facilities.41
* Compared to older adults,
adolescents 10 to 19 years of age and young adults 20 to 24 years of age are at
higher risk for acquiring STIs: they may be more likely to have multiple
(sequential or concurrent) sexual partners rather than a single, long-term
relationship; they may be more likely to engage in unprotected intercourse; and
they may select partners at higher risk.42
http://www.cdc.gov/std/stats/default.htm
Sexually transmitted diseases (STIs)
remain a major public health challenge in the United States. While substantial
progress has been made in preventing, diagnosing, and treating certain STIs in
recent years, CDC estimates that 19 million new infections occur
each year, almost half of them among young people ages 15 to 24.1 In
addition to the physical and psychological consequences of STIs, these diseases
also exact a tremendous economic toll. Direct medical costs associated with
STIs in the United States are estimated at up to $14.1 billion annually.2
This document summarizes 2005 national
data on trends in notifiable STIs — Chlamydia, gonorrhea, and syphilis
— that are published in CDC’s report, Sexually Transmitted Disease Surveillance
2005. These data, which are useful for examining overall trends and trends
among populations at risk, represent only a small proportion of the true
national burden of STIs. Many cases of notifiable STIs go
undiagnosed, and some highly prevalent viral infections, such as human
papillomavirus and genital herpes, are not reported at all.
Chlamydia: Expanded Screening Efforts
Result in More Reported Cases, but Majority of Infections Remain Undiagnosed
Chlamydia remains the most commonly reported infectious disease in the
United States. In 2005, 976,445 Chlamydia
diagnoses were reported, up from 929,462 in 2004. Even so, most Chlamydia cases
go undiagnosed. It is estimated that there are approximately 2.8 million new
cases of Chlamydia in the United States each year.1
http://www.nytimes.com/2005/06/15/health/15pledge.html
Most STD infections are asymptomatic, and therefore, people don't
know that they have an StD unless they get tested. The use of self-report
data for StD's is therefore extremely problematic."
HPV PREVALENCE
CDC study finds more women in the U.S.
have HPV than previously estimated.
Recent data indicate approximately 1 in 4 women in the U.S. have HPV. The prevalence is highest among
younger women in their early and mid-twenties (45%), but remains at a
substantial 20% rate even in the 50-59 year old women.
Prevalence by age was:
• 24.5% ages 14-19
• 44.8% ages 20-24
• 27.4% ages 25-29
• 25.2% ages 40-49
• 19.6% ages 50-59
http://www.ashaSTI.org/news/news_factsheets.cfm
The U.S. has the highest STI rates of any country in the industrialized world. Despite this, there is no national
campaign to promote the prevention, treatment and cure of these infections.
Women STIs are more easily passed from men to women than vice versa, which results in higher female rates of infection.
Each year 9 million new cases of STIs occur among young people aged 15–24. Sexually active youth have the highest STI rates of any age group in the country. By age 25, one-half of all sexually active young people get an STI. Young people are at greatest risk for STIs because, as a group, they are more likely to have unprotected sex and more than one sex partner. Like adults, many teenagers lack awareness of STIs. More than half of all sexually active teens have never discussed STIs with their partner or health-care provider. Young women, in particular, are vulnerable to STIs such as Chlamydia and gonorrhea because of changes in the cervix due to puberty.
Stopping the Spread of STIs Most Americans underestimate
their risk of getting an STI.
According to recent survey data,
only 14 percent of men and 8
percent of women think they are at
risk of becoming infected. u Because the risk is underestimated
— and because many
STIs are “silent” in their early
stages — many people do not get tested and then inadvertently pass the infection to others. u Lack of STI awareness is perpetuated by stigma, secrecy and shame, even between health-care providers and
patients. Over half of all adults and over one-third of all teens in 1995 said
that their health-care providers
spent no time discussing STIs with
them.
An STI Epidemic
http://www.leaderu.com/orgs/probe/docs/epid-STI.html
Sexually Transmitted Diseases (or STIs) are at unprecedented and
epidemic proportions. Thirty years of the sexual revolution is paying an ugly
dividend. While a few STIs can be transmitted
apart from sex acts, all are transmissible by the exchange of bodily fluids
during intimate sexual contact. I want to discuss the severity of the problem
as well as what must be done if we are to save a majority of the next
generation from the shame, infertility, and sometimes death, that may result
from STIs.
The information I am about to share is
from data gathered by the Medical Institute for Sexual Health out of Austin,
Texas.(1) All of these static's are readily available from reputable medical and
scientific journals.
Today, there are approximately 25
STIs. A few can be fatal. Many women are living in fear of what their future
may hold as a result of STI infection. It is estimated that 1 in 5 Americans
between the ages of 15 and 55 are currently infected with one or more STIs, and
12 million Americans are newly infected each year. That's nearly 5% of the
entire population of the U.S. Of these new infections, 63% are in people less
than 25 years old.
This epidemic is a recent phenomenon. Some young people have parents
who may have had multiple sexual partners with relative impunity. They may
conclude that they too are safe from disease. However, most of these diseases
were not around 20 to 30 years ago. Prior to 1960, there were only two
significant sexually transmitted diseases: syphilis and gonorrhea. Both were
easily treatable with antibiotics. In the sixties and seventies this relatively
stable situation began to change. For
example, in 1976, Chlamydia first appeared in increasing numbers in the United
States. Chlamydia, particularly dangerous to women, is now the most common STI
in the country. Then in 1981, human immunodeficiency virus (HIV), the virus
which causes AIDS, was identified. By early 1993, between 1 and 2 million
Americans were infected with AIDS, over 12 million were infected worldwide, and
over 160,000 had died in the U.S. alone. Over 10% of the total U.S. population,
30 million people, are infected with herpes.
In 1985, human papilloma virus (HPV),
began to increase. This virus will result in venereal warts and will often lead
to deadly cancers. In 1990, penicillin resistant-strains of gonorrhea were
present in all fifty states.
By 1992 syphilis was at a 40-year
high. As of 1993, pelvic inflammatory disease (PIV), which is almost always
caused by gonorrhea or Chlamydia, was affecting 1 million new women each year.
This includes 16,000 to 20,000 teenagers. This complication causes pelvic pain
and infertility and is the leading cause of hospitalization for women, apart
from pregnancy, during the childbearing years.
Pelvic inflammatory disease can result
in scarred fallopian tubes which block the passage of a fertilized egg. The
fertilized egg, therefore, cannot pass on to the uterus and the growing embryo
will cause the tube to rupture. By 1990, there was a 400% increase in tubal
pregnancies, most of which were caused by STIs. Even worse is the fact that 80%
of those infected with an STI don't know it and will unwittingly infect their
next sexual partner.
The Medical Facts of STIs
Syphilis is a terrible infection. In
its first stage, the infected individual may be lulled into thinking there is
little wrong since the small sore will disappear in 2 to 8 weeks. The second
and third stages are progressively worse and can eventually lead to brain,
heart, and blood vessel damage if not diagnosed and treated. The saddest part
is that syphilis is 100% curable with penicillin, yet there is now more
syphilis than since the late 1940s, and it is spreading rapidly.
Chlamydia, a disease which only became common in the mid-1970s, infects
20 to 40% of some sexually active groups including teenagers. In men, Chlamydia is usually less serious; with females, however,
the infection can be devastating. An acute Chlamydia infection in women will
result in pain, fever, and damage to female organs. A silent infection can
damage a woman's fallopian tubes without her ever knowing it. A single
Chlamydia infection can result in a 25% chance of infertility. With a second
infection, the chance of infertility rises to 50%. This is double the risk of
gonorrhea.
The human papilloma virus, or HPV, is
an extremely common STI. One study reported that at the
University of California, Berkeley, 46% of the sexually active coeds were
infected with HPV. Another study reported that 38% of the sexually active
females between the ages of 13 and 21 were infected. HPV is the major
cause of venereal warts; it can be an extremely difficult problem to treat and
may require expensive procedures such as laser surgery.
The human papilloma virus can result
in precancer or cancer of the genitalia. By causing cancer of the cervix, this
virus is killing more women in this country than AIDS, or over 4,600 women in
1991. HPV can also result in painful intercourse for years after infection even
though other visible signs of disease have disappeared.
And of course there is the human
immunodeficiency virus, or HIV, the virus that causes AIDS. The first few cases
of AIDS were only discovered in 1981; now, in the U.S. alone, there are between
1 and 2 million infected with this disease. As far as we know, all of these people
will die in the next ten years. As of early 1993, 160,000 had already died.
A 1991 study at the University of
Texas at Austin showed that 1 in 100 students who had blood drawn for any
reason at the university health center was HIV infected. While the progress of
the disease is slow for many people, all who have the virus will be infected
for the rest of their life. There is no cure, and many researchers are
beginning to despair of ever coming up with a cure or even a vaccine (as was
eventually done with polio). In 1992, 1 in 75 men was infected with HIV and 1
in 700 women. But the number of women with AIDS is growing. In the early years
of the epidemic less than 2% of the AIDS cases were women. Now the percentage
is 12%.
Teenagers Face a Greater Risk from
STIs
Teenagers are particularly susceptible
to sexually transmitted diseases or STIs. This fact is alarming since more
teens are sexually active today than ever before. An entire generation is at
risk and the saddest part about it is that most of them are unaware of the
dangers they face. Our teenagers must be given the correct information to help
them realize that saving themselves sexually until marriage is the only way to
stay healthy.
The medical reasons for teens' high susceptibility to STIs specifically
relates to females. The cervix of a teenage girl has a lining which produces
mucus that is a great growth medium for viruses and bacteria. As a girl reaches
her 20s or has a baby, this lining is replaced with a tougher, more resistant
lining. Also during the first two years of menstruation, 50% of the periods
occur with-out ovulation. This will produce a more liquid mucus which also
grows bacteria and viruses very well. A 15-year-old girl has a 1-in-8 chance of
developing pelvic inflammatory disease simply by having sex, whereas a
24-year-old woman has only a 1- in-80 chance in that situation.
Teenagers do not always respond to
antibiotic treatment for pelvic inflammatory disease, and occasionally such
teenage girls require a hysterectomy. Teenage infertility is also an increasing
problem. In 1965, only 3.6% of the married couples between ages 20 and 24 were
infertile; by 1982, that figure had nearly tripled to 10.6%. The infertility
rate is surely higher than that now with the alarming spread of Chlamydia.
Teenagers are also more susceptible to
human papilloma virus, HPV. Rates of HPV infection in teenagers can be as high
as 40%, whereas in the adult population, the rate is less than 15%. Teenagers
are also more likely than adults to develop precancerous growths as a result of
HPV infection, and they are more likely to develop pelvic inflammatory disease.
A study from Florida looked at couples
where one individual was HIV positive and the other was negative. They used
condoms as protection during intercourse. Obviously these couples would be
highly motivated to use the condoms properly, yet after 18
months, 17% of the previously uninfected partners were now HIV positive. That
is a one-in-six chance, the same as in Russian roulette. Not good odds!
Condoms do not even provide 100%
protection for the purpose for which they were designed: prevention of
pregnancy. One study from the School of Medicine Family Planning Clinic at the
University of Pennsylvania reported that 25% of patients using condoms as birth
control conceived over a one-year period. Other studies indicate that the rate
of accidental pregnancy from condom-protected intercourse is around 15% with
married couples and 36% for unmarried couples.
http://www.nlm.nih.gov/medlineplus/ency/article/001949.htm
The following factors increase your risk of getting a
sexually-transmitted disease (STI):
* Not knowing
whether a partner has an STI or not
* Having a
partner with a past history of any STI
* Having sex
without a male or female condom
* Using drugs
or alcohol in a situation where sex might occur
* If your partner is an IV drug user
* Having anal intercourse
Safe Sex
http://www.smartersex.org/safe_sex/safe_sex.asp GOOD
1. Talk smart sex first. Have smart sex later. STIs and unintended
pregnancies affect both partners, not just one person. If you feel
uncomfortable discussing sex and birth control with your partner, then you
shouldn't be having sex. Be straightforward and talk about sex beforehand so
both partners know what to expect. It's easier to be rational and reasonable
before you're in the "heat of the moment."
2. Don't feel pressured to have sex. Or have sex out of fear - fear of
hurting someone's feelings by saying no or fear of being the "only
one" who isn't doing it. Virtually everyone wants to fit in with his or
her friends, but you should never compromise your values to be "part of
the crowd." If you don't want to have sex, be honest, discuss the reasons
behind your decision with your partner and stay true to you.
3. Don't abuse
alcohol/use drugs if you think things could get physical. Drug use or
alcohol abuse interferes with decision-making, which can lead to date rape,
forgetting to use contraceptives or contracting an STI. The lowering of
inhibitions that often accompanies alcohol use might make you think you'll
enjoy sex more, but in fact, for a variety of biochemical reasons, too much
alcohol actually makes sex less enjoyable for both men and women.
4. Two are better than one. To help
prevent both pregnancy and s, you should correctly and consistently
use a birth control method like the Pill, contraceptive injection or diaphragm
(for pregnancy prevention) and a condom (to prevent s). Condom use is
essential, especially in relationships that are not monogamous. If your partner
says no to contraceptives that may prevent s, like condoms, it's probably time
to rethink your relationship. Nothing is worth the potential lifetime
consequences of a few minutes of unprotected fun.
5. Use the buddy
system. If you go to a party or a bar, go with friends and keep an eye
out for each other. Agree that you won't leave with another person without
telling someone. Sometimes a friend's "second opinion" could help prevent
you from making decisions that you might regret later.
6. Remember that
"no" means NO and passed out doesn't mean YES. Being drunk
isn't a defense for committing sexual assault. If you are too drunk to
understand a person trying to say no; if you are too drunk to listen and
respect a person saying no; or if you have sex with somebody who is passed out
or incapable of giving consent, it can be considered rape. Click here to read
about how men and women can avoid the consequences of date rape.
7. Respect everyone's
right to make his/her own personal decision - including yourself. There is no
imaginary "deadline," no ideal age, no perfect point in a
relationship where sex has to happen. If your partner tells you that he
or she is not ready to have sex, respect his/her decision, be supportive and
discuss the reasons behind it. It is everyone's ultimate right to decide when
and how they have sex - be it the first time or the tenth time.
8. Be prepared for a
sex emergency. Consider carrying two condoms with you just in case one breaks
or tears while it's being put on. Both men and women are equally
responsible for preventing s, using contraceptives and both should carry
condoms. Sometimes things go wrong even when you try to do everything right.
Women should also know about emergency contraception or EC. Taken within 72
hours of intercourse, EC may prevent pregnancy. Click here for more information
about EC.
9. The best protection doesn't mean
less affection. Abstinence is actually the most effective way to
protect against s and prevent pregnancy. But practicing abstinence doesn't mean
you can't have an intimate physical relationship with someone - it just means
you don't have vaginal or anal intercourse. There are many other ways to
be intimate and not have intercourse - just be aware that alternatives, like
oral sex, carry their own risks. Click here to read more about practicing
absence and risks of oral sex.
10. Make sexual health a priority.
Whether you are having sex or not, both men and women need to have regular
check-ups to make sure they are sexually healthy. Women should have annual
gynecological exams.
http://www.positive.org/JustSayYes/safesex.html
Nobody has a body to die for. Safe sex
is always better! It's fun, and you don't have to worry as much.
Safe sex means making sure you don't get anyone
else's blood, semen, vaginal fluids, or breast milk in your body -- and protecting your partners too! Condoms, latex surgical
gloves, and plastic wrap are the only ways to protect yourself and your partner
from STIs and HIV, but they're not foolproof. You've got to use them correctly
every time you have sex.
http://en.wikipedia.org/wiki/Safer_sex
Safe sex precautions
* 3.1 Sex by yourself
* 3.2 Non-penetrative Sex
* 3.3 Limiting fluid exchange
* 3.4 Other Precautions
http://en.wikipedia.org/wiki/Non-penetrative_sex
Non-penetrative sex (also known as outercourse) is sexual activity
without vaginal, anal, and possibly oral penetration, as opposed to
intercourse. The terms mutual masturbation
and frottage are also used, but with slightly different emphases. NPS and
outercourse are rather new terms.
No bodily fluids are intended to be exchanged, and outercourse is
therefore often considered a practice of safer sex as well as of birth control (see below for exceptions). Outercourse in preparation for
intercourse can form part of foreplay.
[edit] Support by medical
establishment
Dr. Joycelyn Elders, President Bill
Clinton's surgeon general, tried to popularize outercourse as a means of sexual
play for teens that would offer a safer alternative than sexual intercourse
involving penile-vaginal or penile-anal penetration[2]; however, her
recommendation was opposed by the religious right. Eventually, Elders resigned.
What Outercourse Is and How It Works
There are many ways to be sexual
without intercourse—
Remember: No matter what kinds of sex
play you and your partner choose to have, you both must
* have each other's consent
* never use pressure to get consent
* be attentive to each other's pleasure and
satisfaction — you both have an equal right to sexual pleasure
Advantages for teens
—
Outercourse can completely satisfy
both partners and take a lot of pressure off young women and men.
Many teen women get little or no
pleasure from sexual intercourse because their partners do not know how to give
them pleasure. Outercourse helps partners learn about their bodies and how to
give themselves and each other sexual pleasure.
Women have very different sexual
response cycles than men. Men usually have one orgasm, and it is usually some
time before they can have another. Women can have frequent and multiple
orgasms. But many women don't have orgasms from vaginal stimulation. Most of
them can have orgasms when the clitoris is stimulated — whether or not
they are having vaginal intercourse. Sex play without intercourse can help
women learn how to have orgasms.
Men also enjoy outercourse —
even if they're shy about it in front of their partners. Outercourse allows men
to be truly erotic without worrying about how well they "perform".
Caution — Outercourse is a form
of birth control. It is also a lot like foreplay. They both add to sexual
excitement and pleasure. And they can both lead to orgasm. The difference is
that foreplay usually leads to intercourse. Outercourse may make you feel like
having intercourse. Be careful! If you are going to have intercourse, you need
to use another form of birth control — and protection from infection.
Talking About Outercourse
It is important to talk to your
partner about wanting to enjoy outercourse and abstain from intercourse. But it
may not be easy to do. Here are some tips for talking about outercourse:
* Think about what kinds of sex play you want to
do and don't want to do.
* Practice having a discussion with your
partner. What do you want to say? What are all the possible things your partner
could say?
* Try to have talks with your partner before you
get into a sexy situation.
* Talk when you both have time and privacy for
these discussions.
* Be very clear about the limits you want to
set. Remember that your partner cannot read your thoughts. It's important to
talk about what you want and how you feel. It's important to hear your partner,
too.
* If you are feeling nervous or embarrassed,
tell your partner. Maybe your partner feels the same way you do. Sometimes sex
is hard to talk about. It's okay to say that.
* Ask how your partner feels about outercourse.
Being honest with each other can make a relationship more fulfilling.
* Set limits upon which you both can agree.
* Keep talking about the sexual limits you set
together. What feels good? What may not be working out so well?
* If you decide to have intercourse, be sure you
have another kind of birth control. Also be ready to protect yourself against
infection.
A History of Birth Control Methods
From planned parenthood history of birth control methods
Outercourse
Augune of Hippo (350–430 C.E.), an influential bishop of the early Christian church, taught that
masturbation and other alternatives to penile-vaginal intercourse —
outercourse — were worse sins than fornication, rape, incest, and
adultery. He argued that masturbation and other nonreproductive sexual
activities were "unnatural" sins because they were contraceptive.
Since fornication, rape, incest, and adultery could lead to pregnancy, they
were "natural" sins and much less serious than "unnatural"
sins (Ranke-Heinemann, 1990).
While Augune was compelling all the
married clergy in his diocese to give up their spouses and live celibately in
monasteries (Ranke-Heinemann, 1990), Mallinaga Vatsayayana, in faraway India,
was writing the world's greatest literary celebration of procreative and
nonprocreative sex play — the Kama Sutra, the most complete encyclopedia
of sex practices in the ancient world.
Written in 400 C.E., Vatsyayana's Kama
Sutra is a recapitulation of the Kama Shastras that describes "erotic
practice" as one of the three aims of life for ancient Hindus in India
(Danielou, 1994). The Shastras were already 2,000 years old when Vatsyayana
wrote them in Hindi. More than a thousand years later, the Kama Sutra would
reach across the centuries and have a major impact on us.
The first English translation of the
Kama Sutra was privately published by Sir Richard Burton and discreetly
circulated among the members of the British Kama Sutra Society in 1883. The
first popular publication of this manual for intercourse, foreplay, and
outercourse, which was published in the U.S. during the 1960s, became the bible
for the sexual revolution of that time (Burton, 1991).
In colonial New England, outercourse
was encouraged by the custom of "bundling." Because of the long
distances traveled for courtship and the lack of central heating and bedroom
space, unmarried couples were "bundled." They slept together in the
same bed, either fully clothed or with a "bundling board" placed in
the bed between them. It was assumed that the young people might become
physically intimate, but would refrain from vaginal intercourse. However, the
dramatic rise in the rates of premarital pregnancy and "illegitimacy"
in the middle of the 18th century was blamed on bundling, and the clergy
successfully denounced the practice in 1770 (D'Emilio & Freedman, 1988).
Outercourse had a major revival in America
during the 1940s and 1950s. During those years, virginity was considered very
important for unmarried women. Outercourse in the back seat of her boyfriend's
sedan at the drive-in movies — they were called "passion pits"
by the teenagers of the '50s — allowed a young woman to have sex while
remaining "technically" a virgin (Kinsey, 1948).
Outercourse took a back seat to vaginal intercourse when the pill
became available during the sexual revolution of the '60s (Brandt, 1985; Valdiserri, 1988). By the time the '80s rolled
around, vaginal intercourse was a pretty matter-of-fact event in the
heterosexual "dating game" (Coontz, 1992). But as the sexual
revolution began to lose some of its charm with the spread of AIDS in the early
'80s, many women and men began to wonder if they weren't missing something by
passing up the other pleasures of sex play. Yearning for
romance, and aware of the significant risks of HIV and other sexually
transmitted infections, women and men of the 21st century are rediscovering the
pleasures of courtship, seduction, and outercourse (Cordes, 1988).